
CARPAL TUNNEL SYNDROME
Carpal tunnel syndrome is a painful progressive condition caused by compression of a key nerve in the wrist. It occurs when the median nerve, which runs from the forearm into the hand, becomes pressed or squeezed at the wrist. Carpal tunnel syndrome is more common in women than men.
The carpal tunnel is a narrow, tunnel-like structure in the wrist. The bottom and sides of this tunnel are formed by wrist (carpal) bones. The top of the tunnel is covered by a strong band of connective tissue called the transverse carpal ligament.
The median nerve travels from the forearm into the hand through this tunnel in the wrist.
The median nerve controls feeling in the palm side of the thumb, index finger, and long fingers.
The nerve also controls the muscles around the base of the thumb. The tendons that bend the fingers and thumb also travel through the carpal tunnel. These tendons are called flexor tendons.

Median nerve distribution in the hand.
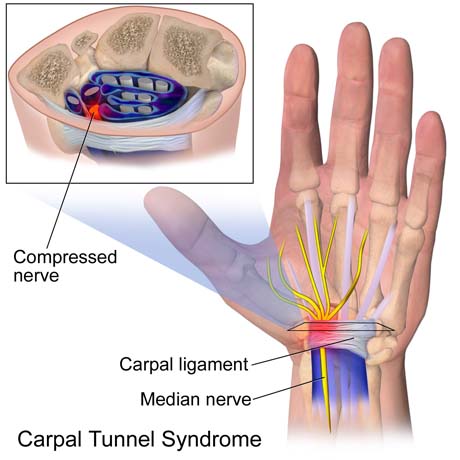
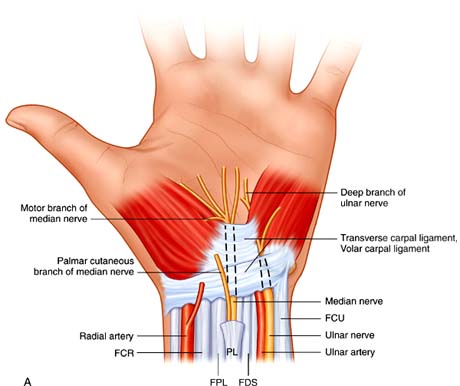
Photo by Operative technique "Hand and wrist Surgery' Chung, Saunders Publication
Cause
Most likely the disorder is due to a congenital predisposition - the carpal tunnel is simply smaller in some people than in others. However, the risk of developing carpal tunnel syndrome is especially common in those performing assembly line work.
In some cases no direct cause of the syndrome can be identified. Sporting activities that predispose athletes to carpal tunnel syndrome include those that involve repititive or continuous extension/flexion of the wrist, as seen in cycling, throwing sports, raquet sports, gymnastic and wheelchair activities.
Symptoms
Patients describe intermittent or persistent numbness and paresthesias mainly affecting the three radial fingers and the radial half of the ring finger.
Pain occurs chiefly at night, causing many patients to awaken in the early morning hours. Many patients report a tendency to drop objects held in the hand (loss of grip strength) or an inability to unlock doors with a key (loss of pinch strength).
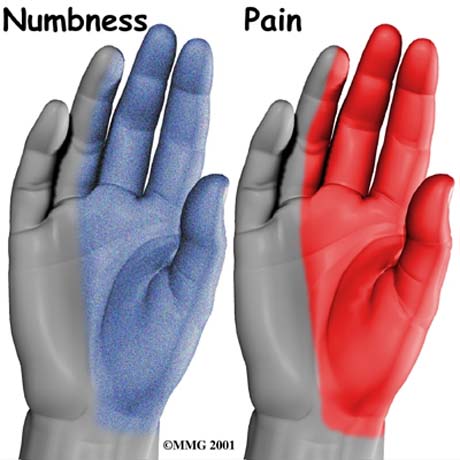
Area of nambness and pain (red area), on hand.

Carpal tunnel syndrome. Thumb muscle atrophy in neglected disease.
How is carpal tunnel syndrome diagnosed?
Early diagnosis and treatment are important to avoid permanent damage to the median nerve. A physical examination of the hands, arms, shoulders, and neck can help determine if the patient's complaints are related to daily activities or to an underlying disorder, and can rule out other painful conditions that mimic carpal tunnel syndrome.
The wrist is examined for tenderness, swelling, warmth, and discoloration.
Each finger should be tested for sensation, and the muscles at the base of the hand should be examined for strength and signs of atrophy. Routine laboratory tests and X-rays can reveal diabetes, arthritis, and fractures.
Plain X-rays often are not helpful in the diagnosis of carpal tunnel syndrome.
Electrodiagnostic studies are necessary to confirm the diagnosis.
Electromyography show evidence of acute or chronic denervation of the thenar musculature.


