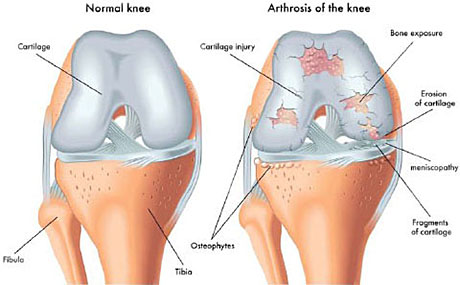
The knee is created by the femur, the tibia and patella. The end surfaces of these bones are covered by articular cartilage that can move one bone relative to another, minimizing friction.
The patella is a bone that is moving in the anterior knee, and over it passes the tendon of the quadriceps muscle and the combination of the patella tendon and creates extensive mechanism of the joint.
The knee is divided on the lateral, the medial and anterior compartment. The lateral compartment consists of the lateral femoral condyle and lateral tibial plateau , the medial compartment of the medial femoral condyle and tibial plateau in through the front end and consists of the patella and femoral trochlea.
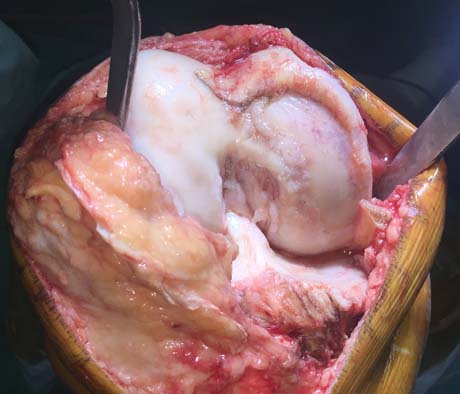
Severe knee osteoartrhitis The osteoarthritic knee
Final stage knee osteoarthritis. The articular cartilage has been completely destroyed
1. Osteoarthritis. is the most common type of arthritis in the knee and is a slow, progressive degenerative <br />
disease in which articular cartilage shows a gradual decay. It starts usually after middle age ends <br />
especially in old age.
2. Rheumatoid arthritis. An inflammatory type of arthritis which destroys the articular cartilage and may occur at any age.
3. Traumatic arthritis. usually occurs after injury to the joint. This type of arthritis is like osteoarthritis and may develop after long periods of a fracture, damage link or tear of the meniscus that was not treated promptly.
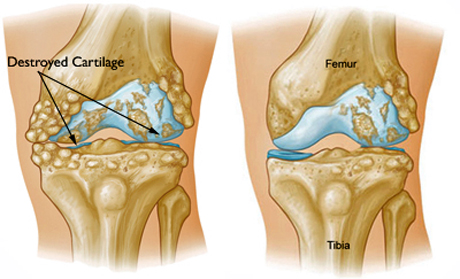
Knee joint with severe degenerative artrhitis. The articular cartilage is damaged.
SYMPTOMS
The pain due to arthritis has been a gradual evolution but the sudden emergence of severe pain may also occur. Usually the symptoms begin with pain after fatigue as the disease progresses and appears calm. The night pain usually means end stage osteoarthritis and surgery is now the only solution.
The affected joint may develop edema (swelling), become stiff, difficult to display in normal flow and range of motion (loss of the last degrees of flexion or extension).
The pain may be the reason why the patient feels weakness in the leg in the early stages. During disease progression by reducing the individual function of the affected joints leads inevitably to the development of muscle atrophy of quadriceps and hamstring muscles having longer objective the reduction of muscle force and occurrence of weakness of the leg.
VISIT TO ORTHOPAEDIC SURGEON
The Orthopaedics Surgeon specialist will examine the knee to determine whether it shows signs of inflammation such as severe edema (swelling), redness and increased local temperature.
Then we will carefully evaluate the scope and quality of motion of joints, it now points to palpation sensitivity occurs if there is fluid in it, we noticed any distortion, the way the patient walks though shows some form of lameness or inability to perform motions.
EXAMINATIONS
X-RAY
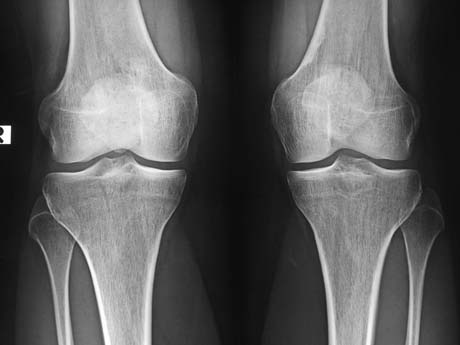
X-ray: normal knee
X-ray: knee osteoarthritis (red circle)
The simple X-ray control shows mainly the reduction of joint space, signifying the loss of articular cartilage and generated spurs. It can also be evaluated and the disturbance of the mechanical axis of the leg.
X-Ray: knee joint with severe degenerative osteoarthritis. There is no cartilage among the bones due to degeneration and this condition produce severe pain.
ULTRASOUND
Ultrasound reveals the knee osteophytes in medial compartment of the knee, suggesting advanced arthritis of the joint
CT- SCANOGRAM
The CT scanogram is the ideal tool for evaluation of anatomical and mechanical axes of the lower extremities, ie the evaluation of the percentage of the derogation and the deformation of the joint than normal.
CT scanogram. Normal mechanical axis of the lower limb
Knee osteoarthritis varus knee, the mechanical axis of the lower limb is not normal CT scanogram: evaluation of mechanical and anatomical axes of the legs to precisely determine the deformation thereof.
MRI
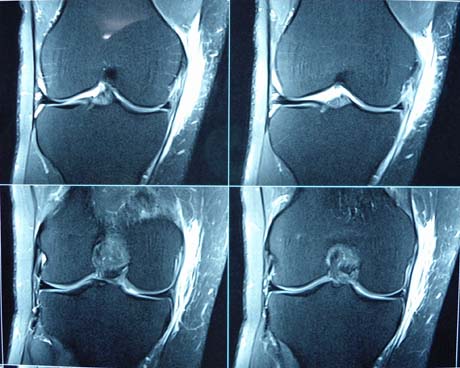
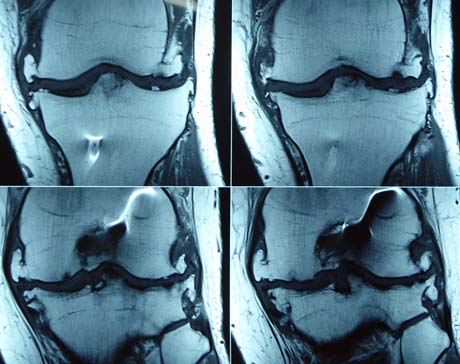
Magnetic resonance imaging helps the physician to a more detailed assessment of the problem by checking the status of articular cartilage, meniscus and ligaments, which will determine the topography of arthritis and the type of treatment to be followed.
MRI knee joint: Normal knee
MRI Knee joint. Severe degenerative osteoarthritis.
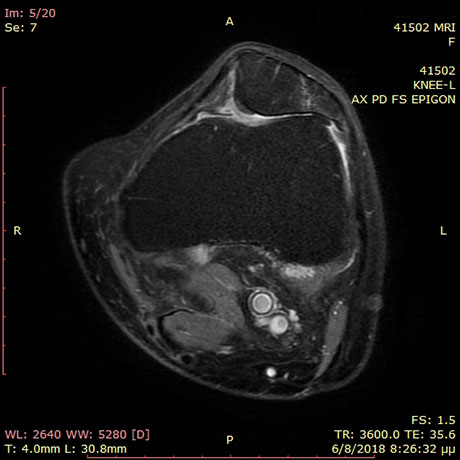
Patellofemoral impingment syndrome. The main patients symptom is anterior knee pain
BLOOD TEST
Specific blood tests will help in the diagnostic process of reasoning of arthritis (rheumatoid arthritis, gout, etc).
Arthroplasty of the knee is one of the most important developments in the history of orthopedics. Today with the help of electronic technology and surgical expertise, the operation of total knee arthroplasty changes page. The new era of application to the patient of customized implants, gives absolute uniformity of materials with specific anatomic particularities of each patient individually who need replacement of the knee joint. The differentiation of the method compared to classical is that the study of each operation carried out before the surgical act with extreme accuracy, evaluating the lower limb as a single anatomical unit correcting the mechanical leg axis which simplifies the process during accomplishment of surgery and promises greater longevity of the implant essentially replacing the surgical navigator.